Download Hypothalamus & Pituitary Gland: Hormones, Disorders, Treatments and more Exams Nursing in PDF only on Docsity!
1
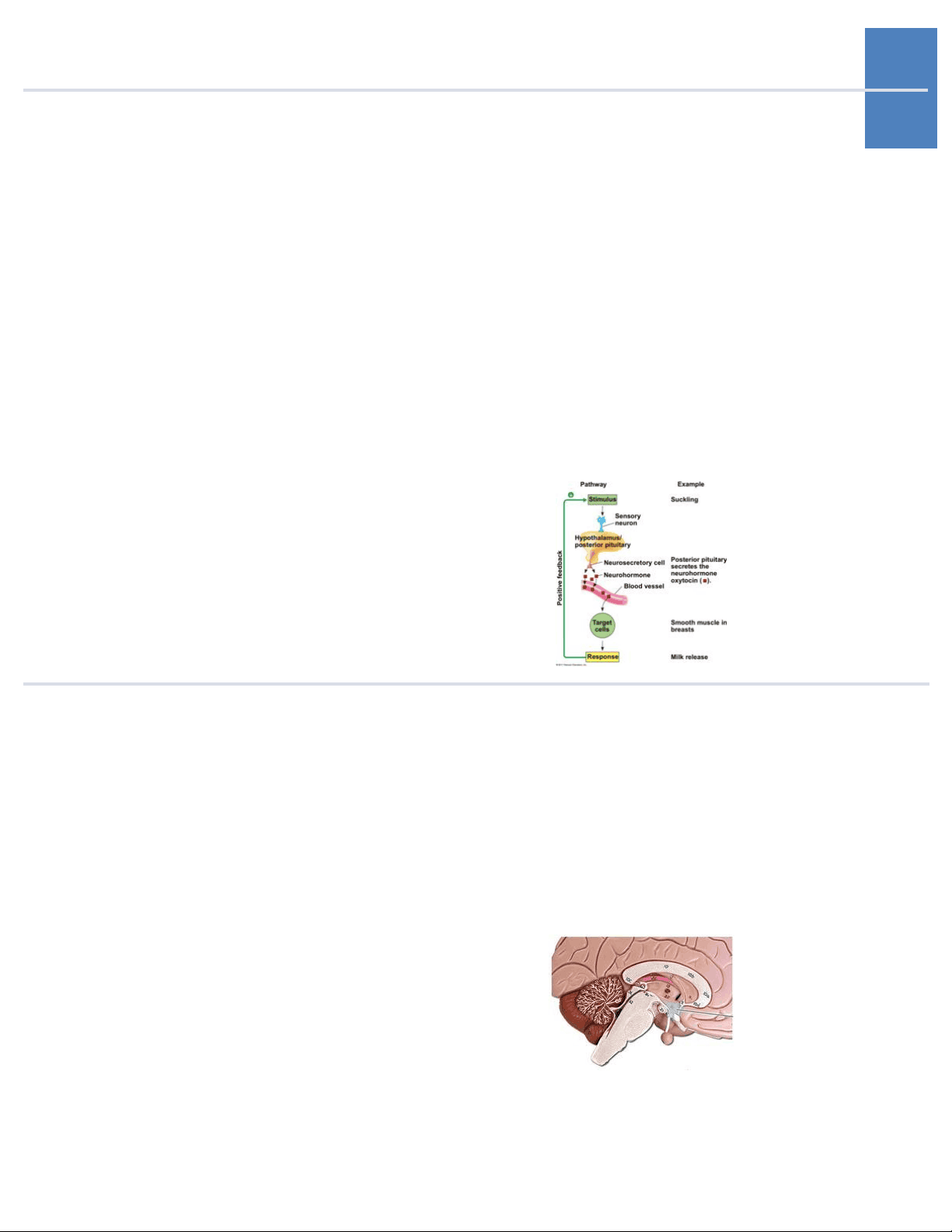
1. Neuroendocrine Sys- tem The endocrine glands that are controlled by and interact with the nervous system; the link between the nervous and endocrine systems. Neurosecre- tory cells = neural cells that release hormones. Remember: there is a direct connection (neu- roectoderm) between hypothalamus and posterior pituitary. Neurosecretory cells of the hypothalamus synthesize ADH and oxytocin and they are trans- ported axonally to the posterior pituitary via the pituitary gland. There is a vascular connection between the hypothalamus and anterior pituitary - neurons end at median eminence where hor- mones enter portal vessels and go to the anterior pituitary where they are secreted.
- Hypothalamus The brain region controlling the pituitary gland. It releases releasing hormones like corticotropin-re- leasing hormone (CRH), thyrotropin-releasing hor- mone (TRH), growth hormone-releasing hor- mone (GHRH), growth hormone-inhibiting hor- mone (GHIH/somatostatin), prolactin-inhibiting hormone (PIH/dopamine), prolactin-releasing hor- mone (PRH), and gonadotropin-releasing hor- mone (GnRH) to the anterior pituitary.
2
- Posterior Pituitary The portion of the pituitary gland, which releases hormones synthesized by the hypothalamus. Neu-
4
6. Corticotropin-Releas- **ing Hormone (CRH)
- Thyrotropin-Releasing** Hormone (TRH) A blood vessel system that directly connects the hypothalamus with the anterior pituitary. Stimulates the release of adrenocorticotropic hor- mone (ACTH) from the anterior pituitary. Stimulates the release of thyroid-stimulating hor- mone (TSH) from the anterior pituitary.
5
8. Growth Hormone-Re- **leasing Hormone
- Growth Hormone-In-** hibiting Hormone **(GHIH/Somatostatin)
- Prolactin-Inhibiting** Hormone **(PIH/Dopamine)
- Prolactin-Releasing** **Hormone (PRH)
- Gonadotropin-Releas-** ing Hormone (GnRH) Stimulates release of growth hormone from the anterior pituitary. Inhibits the release of growth hormone (GH) from the anterior pituitary. Inhibits the release of prolactin from the anterior pituitary. Stimulates release of prolactin from the anterior pituitary. Stimulates the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from the anterior pituitary.
- Oxytocin A hormone released by the posterior pituitary that stimulates uterine contractions during childbirth and milk ejection during breastfeeding. It also stim- ulates smooth muscle contraction in the ductus deferens and prostate gland in males. 14. Antidiuretic Hormone **(ADH/Vasopressin)
- Adrenocorticotropic** Hormone (ACTH) 16. Thyroid-StimulatingHormone (TSH)
7
- Growth Hormone A hormone released by the anterior pituitary that targets all cells in the body. Growth hormone stim- ulates whole body growth in children and adoles- cents, and increases cell turnover rate in adults. It stimulates protein synthesis and growth in bone, muscle, and other tissues.
- Prolactin A hormone secreted by the anterior pituitary that targets the mammary glands stimulating them to produce breastmilk. 19. Follicle-Stimulating **Hormone (FSH)
- Luteinizing Hormone** **(LH)
- Melanocyte Stimulating** Hormone A hormone secreted by the anterior pituitary that stimulates sperm maturation in testes and follicular development and estrogen synthesis in ovaries. Synthesis of inhibin in Sertoli cells of the testes and granulosa cells of the ovaries to act as nega- tive feedback loop to decrease production of this hormone. A hormone secreted by the anterior pituitary that stimulates testosterone synthesis in testes, and will stimulate ovulation, formation of corpus lu- teum, estrogen synthesis, and progesterone syn- thesis in ovaries. A hormone secreted by the anterior pituitary. It stimulates pigment production in the skin.
- Hamartoma Mass of disorganized tissue indigenous to the par- ticular site.
- Hypothalamic Tumors Abnormal growth of hypothalamic neurons leads to asymptomatic, benign growth. It is a problem because of mass effects (pituitary gland adjacent to optic chiasm) and some neurons secrete GnRH,
8 leading to precocious puberty. These tumors can cause hypofunction or hyperfunction of anterior pituitary or combinations. Management: removal vs. GnRH analogues (LH agonists).
10
- Precocious Pseudopu- berty Conditions in which increased productions of sex steroids is gonadotropin-independent. These are tumors of the adrenal gland, ovary, or testes that release high levels of androgens, leading to devel- opment. Occurs before intended release of GnRH. Much less common.
- Precocious Puberty Premature^ onset^ of^ puberty^ with^ the^ appearance of secondary sex characteristics in young children.
11 Due to effect of hypothalamic disease on pituitary function: hypothalamic hypogonadism. Occurs due to early maturation of the entire hypothalamic-pi- tuitary-gonadal (HPG) axis, with the full spectrum of physical and hormonal changes of puberty. Pre- mature activation of the GnRH pulse generator. Defined as onset in < 8 y/o in girls and < 9 y/o in boys. Evaluation: Hx, PE, GnRH stimulation, and MRI. In GnRH stimulation, you need to first collect a baseline level (before stimulation) of LH, FSH, and estradiol/testosterone. Then administer GnRH and measure LH and FSH levels 30 - 60 minutes after stimulation with GnRH. No increase in LH and FSH levels after infusion of GnRH sug- gests precocious pseudopuberty (sex steroids are being produced independently - through adrenal or gonadal tumor). Treatment is through a con- tinuous GnRH agonists like leuprolide (ONLY if it is central cause). This is because prolonged activation of GnRH receptors by this drug leads to desensitization and consequently to suppressed gonadotrophin secretion.
33. Treatment is through a continuous GnRH ag- onists like leuprolide (ONLY if it is central cause). This is because prolonged activation of GnRH receptors by this drug leads to desensiti- zation and consequent-ly to suppressed go- nadotrophin secretion.
13
- Hypopituitarism Condition of diminished hormone secretion from the anterior pituitary gland. It is rare. Etiology: genetic, neoplasms, radiation, vascular, infiltrative disorders, etc. Neoplasms (pituitary microadeno- mas) are the most common cause of acquired hy- popituitarism. It is diagnosed through a Hx and PE
- observe loss of hypothalamic stimulation or direct loss of pituitary function (decreased lab values of pertinent hormones). Stimulate pituitary to pro- duce hormone. Treatment: usually - replace hor- mone physiologically, avoid over-replacement. For example, for pituitary failure to release TSH - give levothyroxine. Monitor dosing: clinical changes +/- based on labs. 35. Usually replace hor- mone physiological- ly, avoid over-replace- ment. For example, for pituitary failure to release TSH - give levothyroxine. Moni- tor dosing: clinical changes +/- based on labs. What is the treatment of hypopituitarism?
- Panhypopituitarism Total/many pituitary impairment that brings about a progressive and general loss of hormone activity.
14
16 42.42.
17 Growth Hormone Defi- ciency (Dwarfism)
43. Growth Hormone Ex- cess (Acromegaly and Gigantism) Absence or deficiency of growth hormone pro- duced by the anterior pituitary gland to stimu- late the body to grow. Leads to dwarfism - an adult high of less than 147 cm (4'-10''). They have normal body proportions, unlike dwarfism caused by achondroplasia. Can be a complete deficiency (slow linear growth rates) or incomplete/acquired (decreased lipolysis, likely do have more adipose tissue). They will have low IGF-1 levels because GH causes its release. Management: GH injec- tions in both children and adults. Increased production of growth hormone. In adults, it is called acromegaly. In children, it is called gigantism (very rare). It is usually caused by a tumor - a GH-secreting pituitary tumor. Symp- toms due to local mass effects depend on the size of the tumor. Can result in bitemporal hemi- anopsia due to pressure on the optic chiasm, HA, and damage to the normal pituitary tissue and can cause deficiencies of ACTH, LH, FSH, and TSH. Symptoms due to excess GH/IGF-1: soft tissue swelling and enlargement of extremities, increase in ring and/or shoe size, hyperhidrosis, coars- ening of facial features, prognathism (protruding jaw), and macroglossia (large tongue). Testing: GH varies during the day. IGF-1 does not vary as much. IGF-1 decreases with age and kidney dis- ease or poorly controlled diabetes and increases with pregnancy. Can perform an oral glucose sup- pression/tolerance test: administer glucose and should observe GH suppression (if normal). In acromegaly, glucose does not suppress GH! Get an MRI and look at pituitary and if nothing seen there, look for ectopic tumors of chest, abdomen, or pelvis. Treatment: trans-sphenoidal surgery =
19
44. Oral Glucose Suppres- **sion Test
- • First-line** = Trans-sphenoidal surgery - Second line = Medications. Use dopamine agonists like bromocriptine and cabergoline. Can also use somatostatin ana- logues like octreotide and lanreotide. also use somatostatin analogues like octreotide and lanreotide. The best confirmatory test for acromegaly. In this test, you give 75g oral glucose load --> should get drop in GH (when normal; don't see the decrease here if acromegaly. What is the first and second-line treatments of acromegaly (adults) and gigantism (children)?
- Hypoprolactinemia A deficiency in the serum levels of the hormone prolactin. It is a rarely a sole deficiency, tends to occur with combined deficiencies. Clinical mani- festation: no postpartum lactation.
- Hyperprolactinemia Excessive prolactin levels. Etiology: pituitary dis- ease including adenoma, hypothalamic disease, medications (antipsychotics MC, ex: risperidone and haloperidol - work by decreasing dopamine). Clinical presentation: in premenopausal women: infertility, oligomenorrhea/amenorrhea, galactor- rhea. Men: hypogonadism, low testosterone - diminished libido, impotence, infertility, rarely galactorrhea. Visual field defects, HA. Medication causes: dopamine-receptor antagonists (metoclo- pramide) or dopamine-depleting agents (reser-
20
48. • In premenopausal women: infertility, oligomenorrhea/amen- orrhea, galactorrhea. - Men: hypogonadism, low testosterone - di- minished libido, impo- tence, infertility, rarely galactorrhea. - Visual field defects, HA. - Medication caus- es: dopamine-re- ceptor antago- nists (metoclopramide) or dopamine-depleting agents (reserpine). - It is diagnosed through measurement of the prolactin level. > 20 ng/mL in men and postmenopausal women. > 30 in pre- **menopausal women.
- Dopamine-receptor** antagonists (metoclopramide) or** dopamine-depleting agents (reserpine).** pine). It is diagnosed through measurement of the prolactin level. > 20 ng/mL in men and postmenopausal women. > 30 in premenopausal women. Treatment: stop the meds that cause it, slow growing tumors - based on symptoms. Bromocriptine is the medication of choice (MOA is to increase dopamine which blocks the release of prolactin). What is the clinical presentation of hyperpro- lactinemia? What medications can cause hyperprolactinemia?