Download Identifying & Treating Fungal Nail Infections in Adults: Dermatology Focus and more Schemes and Mind Maps Dermatology in PDF only on Docsity!
SPECIALITY: DERMATOLOGY
CLINICAL PROBLEM: FUNGAL NAIL INFECTION (ONYCHOMYCOSIS)
These notes should be used in conjunction with the flowchart at the end of this document Introduction Onychomycosis refers to fungal infection of the nails and is one of the commonest dermatological conditions possibly affecting up to 10% of the population. 1 It is more commonly found in toenails (five times more likely) than finger nails. 2
Many people with a long-standing fungal infection of their toenails have no symptoms apart from a change in appearance of the nail characterised by nail thickening and discolouration. In these patients it is entirely appropriate not to treat in order to avoid the additional complications associated with systemic therapy. 3
The purpose of this guidance is to identify the patients in whom treatment is appropriate and the recommended course of action. It should be documented in the patients record that the patient has been informed of the risks associated with treatment.
Causative organism Onychomycosis is an infection of the nail apparatus by fungi that include dermatophytes (responsible for 90% of fungal nail infections) non-dermatophyte moulds and yeasts (mainly candida).^1 Candida infections mainly affect the finger nails. 2,
Symptoms There are different presentations of onychomycosis depending on the infective organism, and each requiring a slightly different treatment course.
Distal and lateral subungual onychomycosis (DLSO) Majority of cases Affects the nail bed (starting at the free end of the nail) Almost exclusively dermatophyte in origin Results in nail thickening, creamy/yellow discolouration and separation of the nail from the nail bed
Superficial white onychomycosis (SWO) Affects the surface of the nail Dermatophyte in origin White discolouration Noticeable flaking
Proximal subungual onychomycosis (PSO) Uncommon No inflammation of surrounding skin Often related to intercurrent disease which may need further investigation e.g. HIV Dermatophyte in origin
Candidal Onychomycosis Chronic inflammation of surrounding skin Nail infection Secondary candidiasis Uncommon
Mould Onychomycosis Occasionally onychomycosis may be caused by moulds such as: Aspergillus, Scopulariopsis, Fusarium, Acremonium Moulds may sometimes show as contaminants in samples. Success of treatment is small and reinfection is high
Investigation
Treatment should not be started on clinical grounds alone.1,3^ When fungal infection is suspected, specimens for confirmation of the diagnosis should be obtained before treatment is started in order to optimise the treatment. 2,
It is estimated that only 50% of nail changes are due to fungal infection 1 , and many other dermatological conditions mimic fungal infection which often accounts for the failure of treatment.^2
The consensus is that investigation of the causative organism and initiation of treatment should only be done in: those with poor or diminished circulation e.g. in diabetics or those with peripheral vascular disease those for whom the infection is causing mechanical problems immunocompromised patients who are at risk of the infection developing into an invasive form. 3
Laboratory diagnosis consists of microscopy to visualise fungal elements in the nail sample and culture to identify the species. Dermatophyte onychomycosis is primarily a disease of the nail bed rather than the nail plate. 1
For samples that show any of the moulds listed under mould onychomycosis a repeat test must be performed as they may just be contaminants in the sample and should therefore not be treated.
In the laboratory the whole of the specimen is examined by microscopy after the addition of 20% potassium hydroxide. The material is then cultured using agar plates which help to identify non-dermatophyte organisms. These cultures can take up to 3 weeks due to the slow growth of dermatophytes.^1
Collecting samples for microscopy If a sample is required then the person must not have taken antifungal treatment within the previous 2 weeks and specimens should be kept at room temperature A dental scraper should be used to scrape material from the underside of the nail and the nail bed from the most proximal part of the nail which yields the best results (the nail may be cut back if necessary, heavy duty nail clippers may be required). For SWO the surface of the nail should be scraped Submit as much material as possible Samples should be put onto black card so that they are clearly visible Ensure all samples are clearly labelled with: the date the sample was taken; area from which the sample was taken; patient details; who has taken the sample, GP/department & address/reference Send the clearly labelled sample for analysis Advise patients that results will take at least 3 weeks
Treatment 3 Before commencing treatment: Consider nail reduction where possible which may improve the efficacy of therapy. Diagnosis should be confirmed by sending samples for mycological examination. Discuss the pros and cons of the treatment with the patient.
See algorithm for treatment guidelines.
In the event of treatment failure the patient should be referred to the specialist dermatologist. Please ensure that copies of the results are sent with the referral.
As results from scrapings take 3 weeks it is unlikely that treatment will be initiated
in the secondary care setting.
Additional Information on Treatment for Onychomycosis for Adults
4,
Drug / Dose
Cautions
Adverse Drug Reactions
Monitoring
Counselling Points
Terbinafine 250mg Tablets 250mg once daily for 6 weeks to 3months (fingernails) 250mg daily for 3 months (toenails– longer than 3 months may berequired)
Hepatic impairment Renal impairment Pregnancy Breastfeeding
GI (nausea, vomiting,diarrhoea, dyspepsia,abdominal pain) Rarely liver abnormalities(hepatitis, jaundice,cholestasis), dizziness,malaise, rash, urticaria,pruritis, taste disturbance,headache, blood disorders(leucopenia,thrombocytopenia)
^ LFT’s ^ FBC’s
^ With
or
without food
Itraconazole 100mg capsules 200mg twice a day for 7 days Finger nails Repeat course after 21 days Toe nails Repeat
course
twice,
allow
days between each course
Hepatotoxicity Acute Liver disorder Cardiac disease Negative inotropicdrugs Pregnancy Breastfeeding
Rarely GI (nausea, vomiting,diarrhoea, dyspepsia,abdominal pain),Hepatotoxicity (jaundice,hepatitis), heart failure,headache, peripheralneuropathy, menstrualdisorders, hypokalaemia,rashes, pruritis and alopecia
^ Monitor liver function ^ Monitor levels in
immunocompromised
^ Renal function^ * Large number of drug
interactions - checkbefore prescribing *
^ With
food, (1-2 hours before
antacids)
^ Patients should be told how
to recognise signs of liverdisease, and advised toseek medical attention ifsymptoms such asanorexia, nausea &vomiting, fatigue, abdominalpain or dark urine develop.
Amorolfine Apply
to
the
affected
nail
once
weekly
Pregnancy Breastfeeding
Slight burning sensation inarea of application. Nail discolouration, brokenand brittle nails
Ensure lunula of nail isfree from mycosis whenamorolfine used alone forincreased rate ofsuccess
^ May
experience
burning
sensation
if^
severe
seek
advice
^ Nail discolouration
No
Ye
s
Mould infection
confirmed
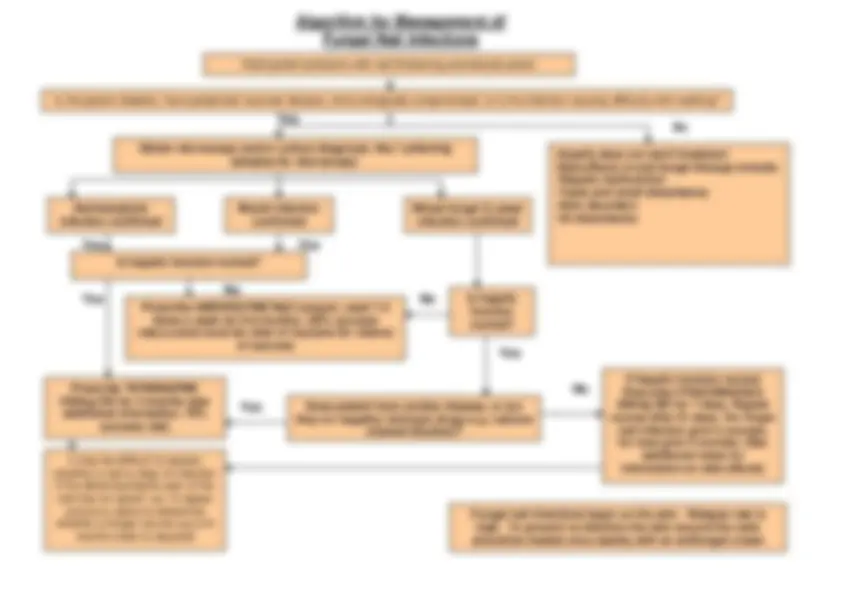
Prescribe AMOROLFINE Nail Lacquer, used 1-
times a week for 6-9 months. (50% success
rate).Lunula must be clear of mycosis for chance
of success
No
Is hepatic function normal?
No
Yes
Yes
Yes
Yes
Obtain microscopy and/or culture diagnosis. See ‘collecting
samples for microscopy’
Usually does not merit treatment Side-effects of anti-fungal therapy include: • Hepatic dysfunction • Taste and smell disturbance • Skin disorders • GI disturbance
Yes
Dermatophyte
infection confirmed
Mixed fungal & yeastinfection confirmed
It may be difficult to assess
whether a nail is clear of infectionif the distal dystrophic part of thenail has not grown out. A repeat
culture is useful to determine
whether a longer course (up to 6
Prescribe TERBINAFINE months total) is required
250mg OD for 3 months (seeadditional information, 70%
success rate)
Is hepaticfunctionnormal?
Does patient have cardiac disease, or are
they on negative inotropic drugs e.g. calcium
channel blockers?
No
If hepatic function normalPrescribe ITRACONAZOLE
200mg BD for 7 days. Repeat
course after 21 days. For finger
nail infection give 2 courses,for toes give 3 courses. (See
additional notes for
information on side effects)
Is the patient diabetic, have peripheral vascular disease, immunologically compromised, or is the infection causing difficulty with walking?
Fungal nail infections begin on the skin. Relapse rate ishigh. To prevent re-infection the skin around the nailsshould be treated once weekly with an antifungal cream
Adult patient presents with nail thickening and discolouration
Algorithm for Management of
Fungal Nail Infections