Download Chapter 1 Rubbins Cellular Adaptation and more Lecture notes Pathology in PDF only on Docsity!
S 01 // T 01 MED2023 1 of 7
Sulcus Widened Gyri narrowed
LEGENDS
Book Knowledge
Powerpoint Information
Sabi ni Doc
Exam (Q&A/LE/PE, Boards)
Clinical Importance ❒ ⌨^ ♪^ ★ ☤ I. INTRODUCTION
Pathology is the study of the structural and functional abnormalities that are expressed as diseases of organs and systems. ❒
If there‟s a persistent sublethal injury cells adapt to injury by decreasing/ceasing function and focus on survival. ⌨ Persistent stress = chronic cell injury For the most part, reversible on discontinuation of stress Severe injury = cell dies. ⌨
II. MAJOR ADAPTIVE RESPONSES
♪ “Take note of each of these adaptive responses - their
characteristics and examples”
A. ATROPHY An active response to an altered environment that results in reduced function or size of cells or organs Decrease in size/weight or function of an organ Dapat i-distinguish ang cellular atrophy sa organ atrophy. Organ atrophy pwedeng resulta ng parehas reversible cell atrophy o irreversible loss of cells. For example, kapag ni-resume ang physical activity ng immobile limb, babalik yung atrophic muscle cells sa usual size and function nila, unlike for example, sa Alzheimer‟s na ang atrophy ay secondary na sa cell death mismo so hindi na kaya ma-restore yung size of the organ. ❒ May be pathologic or physiologic ⌨ May be reversible or irreversible ⌨ Examples: Skeletal muscle atrophy – could be due to disuse or loss of trophic signals of aging Polio - nasisira ang nerve causing atrophy Alzheimer‟s disease – irreversible atrophy of the brain
☤ ♪ On muscle atrophy: “Patients with cast after a few months not using the extremity, mas malaki na yung kaliwa sa kanan pero pag natanggal na yung cast, eventually babalik din sa dati.” Sabi ni doc, this damage is reversible
☤ Difference between Alzheimer‟s and Cerebral Ischemia
♪ Atrophy due to
Alzheimer‟s (right): sulcus widened, gyri narrowed Atrophy of brain is global (entire brain)
★Atrophy due to Cerebral Ischemia (below): Meron kang major blood vessels sa Circle of Willis na nagsusuply sa right side of the brain. Yung blood supply ng right brain mo: either may atherosclerosis or narrowing of lumen compared to the left brain. The blood supply to the brain is regular pero dahil binarahan yung right side the rest of the blood pupunta sa left brain. Kaya yung blood vessels sa left brain ay congested. Assuming pag kinut siya crosswise, dilated ang lumen niya. Compared to alzheimer‟s, in cerebral ischemia, atrophy is only on one side, and the blood vessels are enlarged in the other side.
Causes of Atrophy ⌨ 1 Reduced functional demand (leads to atrophy of disuse) i.e. limb immobilization in a cast → muscle atrophy (reversible) 2 Inadequate supply of oxygen (ischemia) It is frequently seen around the inadequately perfused margins of ischemic necrosis (infarcts) in the heart, brain, and kidneys following vascular occlusion in these organs. ❒ 3 Insufficient nutrients (leads to starvation atrophy) Starvation → atrophy of skeletal muscles and fat. 4 Interruption of trophic signal Endocrine gland ablation or denervation Decreased hormone stimulation.
☤ ♪ “Menopausal women wherein there‟s an absence of estrogen and progesterone you would notice atrophy of endometrial lining even that of the ovaries”
5 Persistent cell injury most commonly caused by chronic inflammation i.e. gastric mucosal atrophy due to chronic gastritis gastric mucosa flattened 6 Increased pressure i.e. decubitus ulcers - bed sores usually seen sa lower back of bed ridden patient 7 Chronic disease Atrophy due to decreased caloric intake i.e. TNF (cachexia) or tuberculosis i.e. Cancer, congestive heart failure, and acquired immunodeficiency syndrome (AIDS) ❒
CELL ADAPTATION, CELL INJURY, AND CELL DEATH
PATHOLOGY (1ST^ Shifting) | (Dr. Alex Florentino) | (Aug. 19, 2020)
Normal Abnormal
(Favorite practical question) Blood vessels of the left side of the brain is congested compensatory effect
Mechanisms of Atrophy ⌨ Increased catabolism of organelles and cytosol reduction → cell shrinkage Organelles and cytosol form autophagic vacuoles Autophagic vacuoles fuse with primary lysosome → enzymatic degradation Undigested lipid stored as lipofuscin Apoptosis (Hindi diniscuss ni Doc pero nasa book, baka importante) Kapag immobilized ang muscle, nangyayari ang “unloading” kung saan nagdedecrease ang contraction kaya mayroon siyang selective adaptive mechanisms. ❒ Protein synthesis – kapag nag-unloading, nagdedecrease ang protein synthesis because of decreased protein elongation by ribosomes which leads to the second adaptive mech; Protein degradation – ubiquitin-related specific protein degradation pathway (i-didiscuss ata „to next meeting) is activated so decreased and contractile proteins. Gene expression - selectively decreased ang gene transcription for contractile activities. “Selective” kasi yung proteins responsible for protein degradation ay expressed pa rin. Signaling – nagbabago yung signals na nagcocontrol for upregulation and downregulation ng intracellular species. Energy utilization – decreased ang free acid utilization as source of energy. B. HYPERTROPHY
An increase in cell size and functional capacity. ⌨ Increased cell size to satisfy increased functional demand ⌨ May be accompanied by hyperplasia Cells capable of division Hypertrophy Hyperplasia i.e. kidney. thyroid Terminally differentiated cells hypertrophy only i.e. heart, skeletal, muscle Associated with initial increase in protein degradation not needed for hypertrophy even as production of proteins that promote hypertrophy increases Cell death is inhibited → increased cell survival
♪ “If you are a gym goer.. What you‟re doing is inducing hypertrophy to your skeletal muscle” Yung mga first timer sa gym, usually first 3 months ang bilis ng weight loss kasi aside from burning the calories merong initial protein degradation. After that, magpaplateau yung weight loss. (Kaya daw a lot of people after 3 mos di na bumabalik sa gym kasi sinasabing nagpaplateau na yung weight loss nila)
Causes of Hypertrophy ⌨ 1 Increased afterload (resistance) or preload i.e. left ventricular hypertrophy (LVH), Cardiac hypertrophy (Exercise), Pathologic hypertrophy due to blocks in the heart 2 Weight training i.e. Skeletal muscle hypertrophy 3 Urethral obstruction i.e. Urinary bladder smooth muscle hypertrophy 4 Removal of one kidney i.e Compensatory hypertrophy (and hyperplasia) of other kidney (which is why individual can live with one kidney)
Mechanisms of Hypertrophy ⌨ The diverse stimuli that lead to cell hypertrophy stimulate adaptive cellular remodeling, increase protein production, facilitate cell function, and promote cell survival. ❒ Endurance training – skeletal muscle (Type I) entails increased aerobic activity (increased oxygen consumption) i.e. marathon runners Resistance training - results in simulation of signaling that does not necessitate increased oxygen supply (Type II) – anaerobic glycolysis i.e. weight lifters
★ ♪ Million Dollar Q & A! What happens to the heart if the hypertrophy is secondary to exercise (physiologic) vs. increased vascular resistance (pathologic)? What makes the hypertrophy due to
exercise physiologic? For both kinds of hypertrophy: ↑↑pumping of the heart myocytes, being muscles, increase in size due to this stress Key difference? Physiologic Cardiac Hypertrophy is due to angiogenesis which is our body‟s physiologic adjustment to exercise. ↑↑ 02 demand (e.g tumatakbo slow steady pace) you need a constant supply of O 2 this endurance training leads to hypertrophy of the myocytes blood carries the O 2 , carried by vessels Ngayon with this endurance training, lumaki ang myocytes mo, lahat ng myocytes mo ngayon nagdedemand ng O 2 arteries sa heart magfoform ng more complex network of capillaries para mas mabilis makapagsupply ng O 2 sa mga myocytes which is absent sa resistance training and sa pathologic hypertrophy (heart diseases) Meanwhile in resistance training you suddenly increase the demand in peripheral muscles without necessarily demanding O 2. Kung ano yung existing blood supply madedeplete lang agad. ☤ So ang marathon runner maraming capillaries madaming O 2 sa heart heart mo hindi na kailangang magpump masyado Result: marathon runners: 50s HR Compared to weightlifter kim bok joo: Highblood (110-120 HR) So therefore, for anyone who will go to the gym, never forget cardio day! Kasi kahit may 6 na pandesal ka pa baka mas healthy pa sayo yung payat na classmate mo na walang ibang ginawa kundi kumain pero hindi nataba.
Cardiac hypertrophy Exercise -physiologic Increased vascular resistance - pathologic Pregnancy – physiologic hypertrophy of the uterus (hormone- induced) Hormone-induced Accompanied by hyperplasia Normal Uterus: 6 x 2 cm
★ FOR PRACTICAL EXAM
When presented with a slide that is obviously a pregnant uterus (see leftmost pic above), it is correct that it is primary/mainly hypertrophy. Correct answer: hypertrophy or hypertrophy and hyperplasia Do not answer “hyperplasia” only (marked wrong)
Effector Pathways for Hypertrophy Kabaliktaran nung adaptive mechanisms kapag atrophy. ❒ Protein degradation - increased Protein translation - increased Gene expression – increased Survival – cell death is inhibited Ancillary function – changes in cells in relation to its environment, such as remodeling extracellular matrix Recruitment of satellite cells – for example, during skeletal muscle hypertrophy, it includes recruiting perimuscular satellite cells to fuse with the muscle syncytia, providing additional nuclei, which are needed to support the expanded protein synthesis needs of enlarging muscle.
Glandular to other types of glandular epithelium i.e. H. pylori → increased goblet cells in pylorus and antrum i.e. intestinal metaplasia Glandular to squamous i.e. smoking – mainstem bronchus epithelium Glandular bronchial epithelium- sensitive to smoke compared to squamous epithelium which can tolerate it i.e. acid pH in vagina vaginal fluid may reflux to endocervical canal metaplasia Transitional to squamous i.e. UB in Schistosoma haematobium infxn i.e. inflamed UB in cystitis glandularis ❒
☤♪ Haematobium: the only species of Schistosoma that lives in the urinary bladder Causes squamous cell carcinoma of the urinary bladder Presentation: hematuria It‟s ova may hook yun ang pinanghohook sa bladder wall mo so naiirritate si transitional epithelium kaya nya kinoconvert to squamous epithelium E. DYSPLASIA
Disordered growth and maturation of the cellular components of tissue ⌨ Reversible Preneoplastic in the sense that it is a necessary stage in the multistep cellular evolution to cancer
Features of Dysplasia ⌨
- Variation in cell size and shape
- Nuclear enlargement. irregularity, and hyperchromatism
- Disarray in arrangement of cells within the epithelium
♪ Dysplasia in epidermis:
Normally, there is maturation from basal layers upward (bottom top) In dysplasia, there is no bottom top maturation
☤♪ CA cell would undergo multiple dysplasia stages before maging CA Dysplasia is preneoplastic in the sense that it is a necessary stage in the multistep cellular evolution to cancer. There is a very fine line between dysplasia and cancer! Parehas ng presentation ang dysplasia and cancer since dysplasia is the morphologic expression of the disturbance in growth regulation. It results from sequential mutations in a proliferating cell population, where the affected cell may predominate when a particular mutation a growth or survival advantage. Their continued proliferation provides greater opportunity for additional mutations, distancing the cell from normal regulatory constraints. However, unlike cancer cells, dysplasia cells are not entirely autonomous and with their intervention. Tissue appearance may still revert to normal. ❒
III. INTRACCELLULAR STORAGE: RETENTION OF MATERIALS
WITHIN CELL
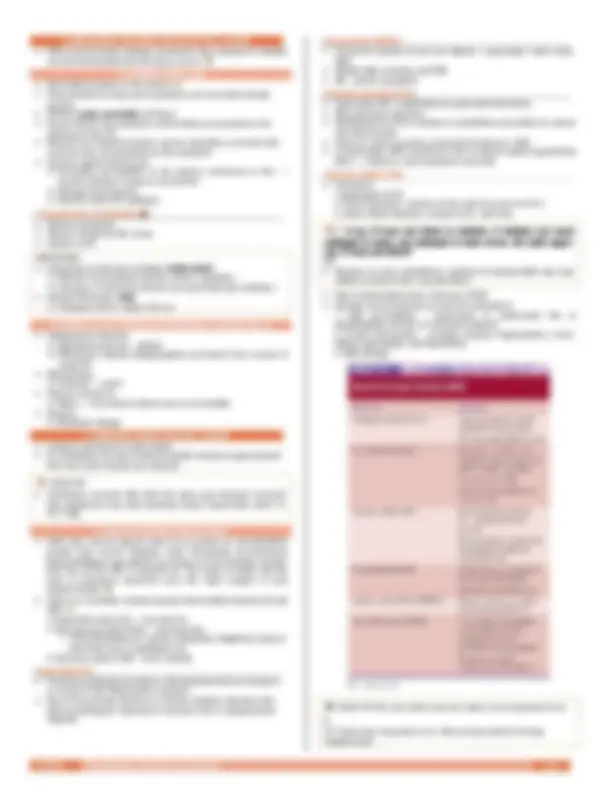
♪ In Calficiations: “Take note the difference between dystrophic “ INJURED” and metastatic “ NORMAL” (keywords!) ★ EXAM TIP! Possible question: clinical situation, tapos ipapaidentify daw kung dystrophic/metastatic
May occur as part of normal development or as a reflection of an abnormal process ⌨ ★ i.e. Calcification of tricuspid valve (right): Lumalabas daw „to sa PE minsan Table 1. Dystrophic vs Metastatic Calcification ⌨ Dystrophic Calcification Metastatic Calcification Macroscopic deposition of calcium phosphate in injured tissue i.e. necrosis – coagulative, liquefactive enzymatic fat Represents an extracellular deposition of calcium from the circulation or interstitial fluid Usually, no functional consequences Normal serum calcium and phosphate Seen in atherosclerosis, chronic pancreatitis May occur in mitral/aortic valves impeded blood flow
Occurs to normal tissue Reflects deranged calcium metabolism that has its origin in cell injury Deposition of calcium phosphate in normal tissue Due to increased serum calcium and/or phosphate
☤♪ HYPERCALCEMIA Causes of Hypercalcemia Increased PTH bone resorption (hyperparathyroidism), ectopic secretion of PTH (malignant tumors) Destruction of bone tissue – primary bone marrow, tumors, skeletal metastasis, accelerated bone turnover (Paget), immobilization Vitamin D-related disorders – intoxication, sarcoidosis, idiopathic hypercalcemia of infancy (abnormal sensitivity to vitamin D) ★♪ Q&A What is the notorious malignant tumor that produces ectopic PTH? Squamous cell carcinoma of the lungs (chronic smokers) Trivia! small cell carcinoma: pumatay kay Merriam Defensor ♪ Trivia! 90% of filipinos are Vit. D-deficient bcoz sa sobrang init sa Pilipinas walang nagbibilad sa araw ♪ May benefit DAW ang Vit. D. supplements sa COVID… ★♪ Q&A Breast Cancer: dystrophic calcification or metastatic? Dystrophic. Why? Because injured tissue na siya ☤♪ HYPERPHOSPHATEMIA Causes of Hypercalcemia Renal failure phosphate retention secondary hyperparathyroidism Primary hypoparathyroidism
IV.MECHANISM AND MORPHOLOGY OF CELL INJURY
When environmental changes exceed the cell‟s capacity to maintain normal homeostasis that cell injury occurs. ❒ A. HYDROPIC SWELLING Reversible increase in cell volume ⌨ Characterized by large, pale cytoplasm and a normally located nucleus Reflects acute, reversible cell injury Excess fluid in the cytoplasm preferentially accumulates in the cisternae of the ER Results from impaired cellular volume regulation, a process that controls ionic concentrations in the cytoplasm. Injurious agents interfere by : Increasing permeability to the plasma membrane to Na+ → exceed capacity of pump to extrude Na+ Damage pump directly Interfere with ATP synthesis
3 Components of Regulation ⌨ Plasma membrane Plasma membrane Na+ pump Supply of ATP
IMPORTANT! Component of hydropic swelling: mainly water! Results from impaired cellular volume regulation
Any injury of the three (above) can cause hydropic swelling ♪
(Recall) Mnemonic: PISO Potassium (K) in, Sodium (S) out
B. SUBCELLULAR CHANGES IN REVERSIBLY INJURED CELLS Endoplasmic reticulum Distended cisternae – dilated Ribosomes undergo disaggregation and detach from surface of rough ER Mitochondria Ischemia → swell Plasma membrane Blebs → may detach without loss of cell viability Nucleus Nucleolar change V. OXIDATIVE STRESS AND CELL INJURY Leads to cell injury in many organs O 2 metabolism can also produce partially reduced oxygen species that react with virtually any molecule.
★ EXAM TIP! Familiarize yourself with both full name and chemical formula? Pag nagpaexam daw kasi pwedeng buong “Superoxide anion” or “O 2 - “ lang
A. REACTIVE OXYGEN SPECIES (ROS) Cells also may be injured when O 2 is present at concentrations greater than normal. Madalas under therapeutic circumstances kapag binibigyan ang patients ng oxygen at concentrations greater than the normal 20% of inspired air. The lungs of adults and the eyes of premature newborns were the major targets of such oxygen toxicity. ❒ There are 3 partially reduced species intermediate between O2 and H2O ⌨
- Superoxide anion (O 2 - ) – one electron
- Hydrogen peroxide (H 2 O 2 ) – two electrons Trivia! Glutathione is a potent antioxidant. Nagkataon lang na side effect nya ay nakakaputi sya.
- Hydroxyl radical (•OH) – three radicals
Superoxide (O 2 - ) Produced principally by leaks in mitochondrial electron transport or as part of the inflammatory response One of the principal effectors of cellular oxidative defenses that destroy pathogens, fragments of necrotic cells or phagocytosed material
Peroxynitrite (ONOO-) Formed by reaction of two free radicals – superoxide + nitric oxide (NO) Attacks lipid, proteins, and DNA NO – potent vasodilator Hydrogen peroxide (H 2 O 2 ) Superoxide (O2-) catabolized by superoxide dismutase Not particularly injurious Metabolized to H 2 O by catalase or glutathione peroxidase in cytosol and mitochondria However, when in excess, converted to hydroxyl (•OH) In neutrophils, MPO transforms H 2 O 2 to potent radical hypochlorite (OCl-) → lethal for microorganisms and cells Hydroxyl radical (•OH) Formed by:
- Radiolysis of H 2 O
- Fenton Reaction: reaction of H 2 O 2 with ferrous iron (Fe 2 +)
- Haber-Weiss Reaction: reaction of O 2 -^ with H 2 O 2
★♪ X-ray, CT-scan and others is radiation. If radiation can cause radiolysis of water, and radiolysis of water forms •OH, bakit nagxx- ray, CT scan and others? &A Because we have glutathione, catalase na kayang ifight ang mga radical na naform ng x-ray and others Most reactive/destructive molecule of ROS Damage macromolecules by several mechanisms:
- Lipid peroxidation – destruction of unsaturated FAs of phospholipids and loss of membrane integrity
- Protein interactions – proteins undergo fragmentation, cross- linking, aggregation, and degradation
- DNA damage
★ EXAM TIP! Doc love tables and can make a lot of questions from it. (♪ ”Aralin niyo „tong table na „to. Dito pa lang madami na kong maitatanong”)
Tattoos Introduction of insoluble metallic and vegetable pigments into the skin, where they are engulfed by dermal macrophages and persist for a lifetime.
☤♪ “Kaya pag tumatagal, kumukpas yung tattoo, dahil don sa macrophages…”
G. IRON AND OTHER MATERIALS Iron – stored intracellularly as ferritin liver and bone marrow are rich in ferritin, although it is present in all cells. ❒ Iron overload syndrome – severe deposition organ damage, including heart, liver, and pancreas, mas extreme kumpara sa hemodiserosis Hemosiderin – partially denatured form of ferritin; yellow-brown granules in cytoplasm found mainly in the spleen, bone marrow, and Kupffer cells of the liver Hemosiderosis – progressive accumulation of hemosiderin kapag dinamihan ang total body iron ng katawan does not injure cells found in the skin, pancreas, heart, kidneys, and endocrine organs ❒ Hereditary hemochromatosis – genetic abnormality in iron absorption ❒ Lead accumulation in children mental retardation, anemia Copper Wilson disease – hereditary disorder of copper metabolism Copper accumulate in liver and brain
VIII. PRACTICE ;) ★ 1 Best neutralizer for hydroxyl free radical? 2 Damaged Na-K-ATP pump effect on NA and K concentrations?. 3 Excess of H 202 is converted to what? 4 Major adapative response wherein tissue assumes phenotype that provides it w/ the best protection from the insult? 5 What best describes metastatic calcification? 6 What cellular process could possibly contribute to an increase of uterine in size? a. Endometrial glandular hyperplasia b. Endometrial stroma hypertrophy c. Myometrial hyperplasia d. Myometrial hypetrophy 7 Ovarian mass revealed papillary tumor with round laminated calcifications. What could this be? a. Abscess formation b. Dystrophic calcification c. Metastatic calcification
ANSWERS:
- Ascorbate
- Increase Na inside, increase K outside
- Hydroxyl radical
- Metaplasia
- Accumulation of calcium phosphate in normal tissues
- Actually di ko rin sure, pero B ata. Search niyo na lang hehe
- Dystrophic calcification
VII. REFERENCES
Rubin's Pathology Clinicopathologic Foundations of Medicine (6th Ed) Doc Alex‟s PPT (2020) Cell Adaptation, Cell Injury, and Cell Death C2: Note-takers (Jelly, Jessa) C4: Listeners (Paeng, Cathy, Xavi) C3: Visual (Tara) C1: Abs, Diocell F